Continuous Palliative Sedation in Paediatric End-of-Life Care: Czech Physicians' Practices and Attitudes
Ms. Anna Tučková, Centre for Palliative Care, Czech Republic. Dr. Kristýna Poláková, Lancaster University, Institute Pallium, Czech Republic Ms. Hana Fischer, School of Human Medicine, University of Zurich Faculty Medicine, Switzerland Ms. Jitka Kosíková, The Czech Society of Palliative Medicine, Czech Medical Association of J. E. Purkyně, Czech Republic Prof. Kim Beernaert, End-of-Life Care Research Group, Vrije Universiteit Brussel (VUB) & Ghent University, Belgium
Background
Continuous palliative sedation (CPS) is a complex medical intervention used to relieve refractory suffering in patients at the end of life. While widely accepted in adult care, its application in paediatrics presents unique ethical and clinical challenges, particularly regarding decision-making involving minors and the distinction between sedation and euthanasia. International discourse emphasises the importance of physician training and experience in navigating these sensitive scenarios. However, data on the specific practices, dosing strategies, and ethical perceptions of physicians in Central Europe, particularly within the Czech Republic, remains limited. Understanding how clinical background influences the administration of CPS is crucial for developing standardized guidelines and ensuring patient safety.
Aim
The primary objective of this study was to investigate the experiences, clinical practices, and ethical attitudes of Czech physicians regarding continuous palliative sedation in paediatric patients. Specifically, the research aimed to identify correlations between physician demographics, level of palliative care training, and direct experience with CPS on one hand, and their clinical decision-making, dosing preferences, and ethical perceptions on the other. The study sought to determine whether specific subgroups of physicians—such as those with paediatric palliative care experience versus general paediatricians, or those with extensive training versus none—demonstrate significantly different approaches to this end-of-life intervention.
Methods
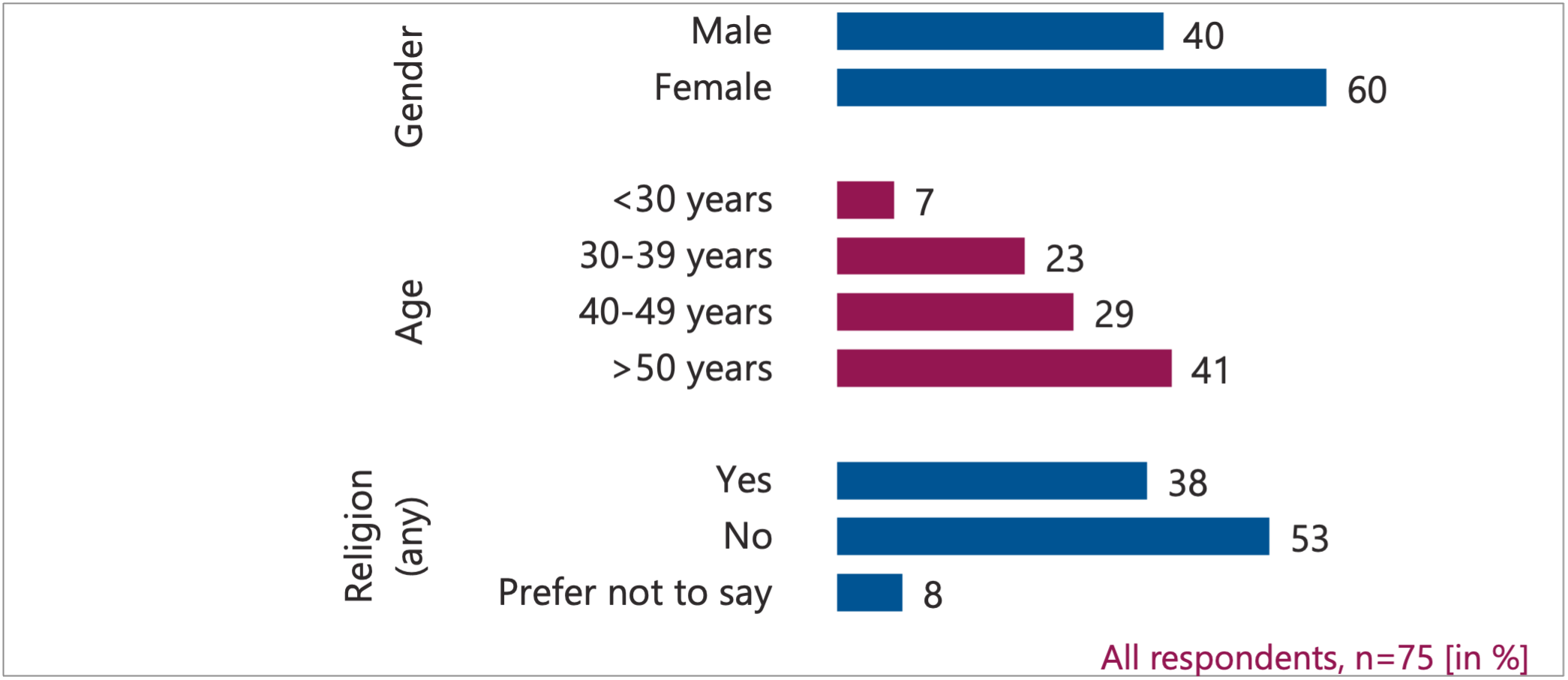
This study utilised a cross-sectional survey design as part of a larger international research project involving Belgium, the Netherlands, Switzerland, Portugal, and the Czech Republic. Data were collected via an online questionnaire distributed through national medical associations. The final sample consisted of 78 physicians, with 75 valid responses retained for analysis after excluding three incomplete entries.
The instrument assessed demographic variables (age, gender, religious affiliation), professional characteristics (specialisation, years of practice, board certification), and specific experiences with CPS over the preceding 12 months. Participants were asked about the frequency of CPS administration, medications used, dosing strategies (gradual titration vs. high initial dose), and the perceived goals of the procedure. Additionally, the survey included hypothetical scenarios to gauge ethical attitudes regarding the acceptability of CPS for various types of suffering, the distinction between CPS and euthanasia, and the impact of CPS on the dying process. Statistical analyses focused on identifying significant differences between groups defined by their clinical specialisation, experience with CPS, and level of palliative care training. Data were analysed using descriptive statistics, chi-square tests, and ANOVA (<0,05).
Results
The largest clinical group was general paediatrics (41%), followed by paediatric intensive care (16%) and neonatal intensive care (10%). A significant portion of respondents (58%) reported having direct experience with administering CPS, while 42% had none.

Number of respondents with experience with CPS.

Number of patients with CPS in last 12 month.
Impact of Paediatric Palliative Experience A clear divergence in clinical practice emerged based on experience with paediatric palliative patients. Physicians who had cared for children in end-of-life settings demonstrated distinct dosing preferences compared to those without such experience. Specifically, those with paediatric palliative experience were significantly more likely to initiate CPS with a high dose to achieve a rapid onset of effect. In contrast, physicians lacking this specific experience predominantly favoured a strategy of gradual titration, starting with low doses and increasing slowly. Furthermore, regarding the goals of sedation, physicians with paediatric palliative experience were significantly more likely to view the induction of unconsciousness as an acceptable or intended outcome of CPS. Those without this experience were more hesitant, viewing unconsciousness primarily as a side effect rather than a therapeutic goal.

Impact of Direct CPS Experience Direct experience with administering CPS also shaped ethical perception. Physicians who had performed CPS were significantly more likely to acknowledge that the procedure can shorten the dying process. While 43% of the total cohort disagreed that CPS shortens life, this disagreement was less prevalent among those with hands-on experience. Conversely, physicians without CPS experience expressed higher levels of uncertainty, with a larger proportion selecting "I don't know" when asked about the impact on the duration of life. Additionally, experienced physicians were more likely to report that the relief of parental suffering is a secondary, yet relevant, motivation for the procedure, alongside the relief of patient suffering.

I consider that the continuous use of sedatives in the last hours to days of life shortens the duration of the dying process.
Role of Palliative Care Training The level of specialised training emerged as a critical factor influencing both clinical confidence and ethical clarity. A concerning finding was that 31% of all respondents, and notably one-third of those actively administering CPS, had received no specialised training in palliative care. Physicians with more extensive training (greater than one day) demonstrated significantly higher confidence in distinguishing CPS from euthanasia in clinical practice (92% vs. 54% for those with minimal or no training). This group also held more conservative views regarding the timing of the intervention, being significantly more likely to deem the use of "premature" CPS to control physical symptoms as unacceptable. In contrast, physicians with limited or no training exhibited greater variability in their ethical stances and were less certain about the boundaries of the procedure.

I feel that in clinical practice the continuous use of sedatives in the last hours to days of life can be difficult to distinguish from euthanasia.
Medication and General Attitudes Regarding pharmacological choices, opioids (36%) and midazolam (35%) were the most frequently used agents. Overall, 99% of physicians considered CPS acceptable for relieving severe physical suffering at the end of life, while acceptance dropped to 56% for psychological distress occurring weeks before death. Eighty-five percent of respondents viewed death in a CPS-induced sleep as a "good death." However, nearly 20% expressed concern that CPS might not adequately relieve suffering in all patients, even after the patient became unresponsive.

The most common medications used for CPS. More options were possible to choose.
Discussion
The findings of this study underscore that clinical background is a primary determinant of how continuous palliative sedation is practiced and perceived. The data reveals a distinct stratification in medical practice: physicians with direct experience in paediatric palliative care who have experience with CPS tend to adopt more direct, rapid-acting dosing strategies and are more comfortable with the goal of inducing unconsciousness. This suggests that exposure to the acute realities of paediatric end-of-life suffering fosters a clinical approach prioritising immediate symptom relief, potentially viewing the speed of onset as a critical component of ethical care.
Conversely, physicians without this specific experience (physicians with background in adult palliative care) tend to favour gradual titration and express greater hesitation regarding the induction of unconsciousness. This caution may stem from a lack of familiarity with the urgency of refractory symptoms in dying children or from a stronger adherence to theoretical ethical constraints that prioritize the preservation of consciousness. The correlation between experience and the acknowledgment that CPS may shorten the dying process further highlights how clinical reality shapes ethical understanding; those who have witnessed the procedure are more likely to recognize its physiological effects, whereas those without experience remain uncertain.
The role of education is perhaps the most significant implication of this research. The finding that a substantial proportion of physicians administer CPS without specialised training represents a threat to ethical consistency and could be a potential risk for patient safety. The data clearly shows that structured palliative care training enhances a physician's ability to distinguish CPS from euthanasia, reduces uncertainty regarding the procedure's impact on life duration, and promotes more consistent clinical decision-making. The gap in training is particularly acute given that one-third of active practitioners lack formal preparation.
In conclusion, the variation in practices and attitudes observed in this cohort indicates that current educational frameworks may be insufficient for preparing physicians for the complexities of paediatric CPS. To ensure high-quality, safe, and ethically sound care, there is an urgent need for enhanced, mandatory training programs. These programs should specifically address the nuances of paediatric end-of-life care, clarify the ethical boundaries between sedation and life-shortening interventions, and provide standardised protocols for dosing and decision-making. By aligning clinical practice with robust educational foundations, the medical community can improve confidence and consistency across all physician groups, ultimately benefiting the vulnerable paediatric population at the end-of-life care.